Hans Selye (1907-1982) The father of the study of stress
He developed the idea that there is a direct relationship between stress and excessive wear and tear throughout the body.
1.Definition of Stress
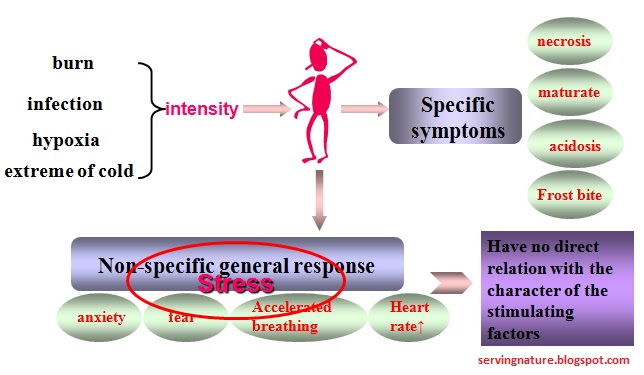
Selye described stress as “ a state manifested by a specific syndrome of the body developed in response to any stimuli that made an intense systemic demand on it.”
Defined as a state of tension that can lead to disharmony or threaten the homeostasis of body.
The current concept of stress is “Non-specific response of the body to any demand made upon it.”
Characters of stress
Non-specific response
Influenced by some factors
Double significance of stress
eustress >> increase mental and physical alertness, enhance adaptative abilities
distress >> disease (peptic ulcers, cardiovascular disease, psychosomatic disease)
2. Stressor
Any stimuli ,or demands ,on body that exceeds a threshold and causes stress response are stressors.
Exogenous stressor
Noise, trauma, infection, cold, heat, pollution,
Endogenous stressor
Alternation of blood compositions, disturbance of homeostasis
Mental-social stressor
Competition, overcrowding, loneliness ,great pressure of work
Acute Stress
Acute stress is the reaction to an immediate threat, commonly known as the fight or flight response
Common acute stressors include:
noise, crowding, isolation, hunger, danger, infection, and imagining a threat or remembering a dangerous event.
Under most circumstances, once the acute threat has passed, the response becomes inactivated and levels of stress hormones return to normal, a condition called the relaxation response.
Chronic Stress
Frequently, however, modern life poses on-going stressful situations that are not short-lived and the urge to act (to fight or to flee) must be suppressed. Stress, then, becomes chronic.
Common chronic stressors include:
on-going highly pressured work, long-term relationship problems, loneliness, and persistent financial worries.
3.General Adaptation Syndrome
- General because the effect was a general systemic reaction no matter what stressor is
- Adaptation because the response was in reaction to a stressor in order to maintain homeostasis
- Syndrome because the physical manifestations were coordinated and dependent on each other.
Stages of GAS
The body passes through three universal stages of coping.
First there is an "alarm reaction," in which the body prepares itself for "fight or flight." No organism can sustain this condition of excitement.
Second stage of adaptation ensues (provided the organism survives the first stage). In the second stage, a resistance to the stress is built.
Finally, if the duration of the stress is sufficiently long, the body eventually enters a stage of exhaustion, a sort of aging "due to wear and tear."
Mechanism-stress response
Neuroendocrine response
1. Locus ceruleus-nor-epinephrine (LC/NE) /sympathetic-adrenal medulla axis
2. Hypothalamic-pituitary-adrenal cortex
(HPA) axis
Humeral response--- Acute phase response
Increase of Acute phase protein in plasma
Cellular response
Up-expression of heat shock protein
1. Neuroendocrine Response
The essential function in stress response
(1)Locus ceruleus-norepinephrine (LC/NE) /
sympathetic-adrenal medulla axis
The essential function of
LC/NE- sympathetic/ adrenal medulla axis
The effects of the increased catecholamines and sympathetic activity
positive effects
1.Heart function increased: Heart rate↑ ,myocardial contractility ↑
cardiac output ↑, blood pressure ↑ → Blood supply to tissues ↑
2. Blood redistribution →kidney, skin, viscera receive a decreased blood supply >
heart, brain, and skeleton muscles receive an increased blood supply
3.Breathing rate↑, bronchodilation →alveolar ventilation ↑,oxygen supply ↑
4.glycogenolysis →blood glucose level ↑
lipolysis → blood fatty acids level ↑ →energy substrates supply ↑
5.Regulate other hormone level: growth hormones(GH)↑, thyroxine ↑,
glucagon ↑, and CRH (corticotropin releasing hormone)↑, insulin↓
negative effects: Hypertension, stress ulcer, visceral ischemia
(2)Hypothalamic-pituitary-adrenal cortex (HPA) axis
The essential function of HPA axis
In central: CRH act as a neurotransmitter within the CNS.It can modulate learning, memory, emotion, etc
- low doses of CRH promote adaptation →
- excitation or pleased feeling
- high doses of CRH cause maladaptation →
- anxiety, depression, and inhibition of feeding,growth
- CRH→ACTH →GC
- CRH →promote LC-NE neuron →activate LC-NE axis
In peripheral: GC is the final effector of the HPA axis, and plays a key role in the regulation of stress
- Increased GC will protect the organism against the effects of stressor.
- Excess GC will exert detrimental effects on body
The positive effects of the increased GC
1.GC maintains blood glucose levels by antagonizing the effects of insulin and enhances the glycogenolysis 2. GC provides fundamental supports for many other hormones (CA, GH, glycocargon)----“permission roles” 3. GC can stabilize lysosomal membrane and lessen tissue damage 4. GC also suppress inflammation and anaphylaxis
All of these functions can protect the organism against the effects of stressor, and focus energy on regaining homeostasis.
The negative effects of the increased GC
Negative effects
- alteration of metabolism→negative nitrogen balance
- Suppress immune response → infection
- Suppress thyroid axis → delayed growth
- result in hormonal resistance → delayed growth
- Suppress gonad axis → delayed development
Note: Person with prolonged stress trend to manifest infection, mental depression, increased incidence of peptic ulcer, delayed growth and development.
Alterations of other hormones in stress
2.Humoral stress response
Acute phase response: is a quick mobilized non-specific immune response against infection, injuries and variety of noxious stimuli, which manifests elevation of WBC count, increase of acute phase protein , etc.
Acute phase protein (APP): are a group of plasma proteins which concentrations in plasma increase quickly upon the acute stress.
APP represents an important adaptive, protective mechanism in humoral level.
Classification and function of APP
C-reactive protein and complements: raise the eliminating power for infectious agents, necrotic debris, increase anti-infection and anti-injury capacity of body .
Protease inhibitors---α1-antichymotrypsin and α1-antitrypsin: protect the tissue from injury by protease
Coagulating proteins--- fibrinogen: enhance the hemostatic power of body against hemorrhage
Ceruloplasmin: eliminate oxygen free radical, protect body against oxidative stress injury.
3.Cellular stress response
Heat shock protein(HSP): are a family of stress protein whose synthesis is up-regulated in response to a variety of stressors.
Up-expression of HSP during stress represents an important adaptive and protective mechanism in cellular and molecular level.
Classification of HSP
HSPs subfamily:HSP110,HSP90,HSP70,HSP60, HSP40,small HSP20, and ubiquitins
Function of HSP
■ The primary role of the HSP----- assist protein folding and repairing in vivo, “Molecular chaperone”
In normal, HSP accelerate proper folding of newly synthesized proteins, guide them translocation and assembly
Under stress conditions, HSP associate with damaged proteins, prevent their abnormal binding with other macromolecules and refold the damaged proteins.
■ Maintain the homeostasis in vivo : degrade and remove bad-damaged and unreparable protein
Functional and Metabolic Alteration
- Central nervous system
- Immune system
- Cardiovascular system
- Digestive system
- Genito-urinary system
- Metabolic alteration
Central nervous system (CNS)
1-CNS is the regulation center of stress response.
Without the sensation, recognition, integration, and interpretation by CNS, many stress will not happen, such as social psychology stress .
2. CNS is effected by stress response.
The moderate stress response will do profit to memory, concentration, and learning.
The hypo-arousal or hyper-arousal of CNS are both distress state, which may cause depression, sadness, or anxiety, panic, etc.
Immune system
1. Immune system is an internal sensory organ that recognizes non-cognitive stimuli such as bacteria, viruses, and other antigens, and relays information to the neuroendocrine system via hormones secreted by immunocytes.
The primary Hormones secreted by immunocompetent cells
2. the stress neurohormones have significant impacts on immune system.
■ the acute stress enhances the no-specific immune function, the number and activity of phagocytes increases, complements, C-reactive protein levels raise, and there is a brief period of immunopotentiation.
■ But the prolonged stress, variety of distresses are associated with immunosuppression, disturbance of immune system, even autoimmune diseases.
Cardiovascular system
Digestive system
Genito-urinary system
The reproductive system is inhibited: The signs are typically manifested in ladies upon strong stress, such as menstrual disorder, amenorrhoea, or dysgalactia, galactostasis in breast feeding women, decreased libido, and impotence.
Metabolic Alteration
The metabolic demands significantly increase upon stress
catabolism increase, anabolism decrease, metabolic rate increase significantly.
Stress and diseases
stress disease
Directly caused by severe noxious stressors. Stress ulcer is a prototype of stress disease.
stress related disease:
Stress is an involving factor, which may participate or intensify the attack of development of the diseases as a risk factor or precipitating factor. Such as hypertension, post-traumatic stress disorder (PTSD), et al.
Stress Ulcer
Mucosal damage or lesion of the stomach or duodenum in critical illness or severely stressed situation, such as severe burning, trauma, hemorrhage, respiratory failure, sepsis, and so on.
Incidence of stress ulcer in critical patients:75%~100%
Develop within 72 hours after a great insult
Manifestation: mucosal erosion,
superficial and multiple ulcer、errhysis. Few ulcer may occur life-threatening hemorrage or perforation. Most of them recovery without any sequela.
Mechanisms of stress ulcer
1.gastrointestinal mucosal ischemia; the basic pathogenic mechanism
2.counter-diffusion of gastric hydrogen ion to mucosa; the major injurious factor for stress ulcer
Post-Traumatic Stress Disorder Symptoms
Post-traumatic Stress Disorder is a psychiatric disorder that can occur following the experience or witnessing of life-threatening events such as military combat, natural disasters, terrorist incidents, serious accidents, or violent personal assaults, like rape.
People who suffer from PTSD often relive the experience through nightmares and flashbacks, have difficulty sleeping, and feel detached or estranged, and these symptoms can be severe enough and last long enough to significantly impair the person's daily life.
Gastrointestinal Problems
(Irritable bowel syndrome,
Crohn's disease or ulcerative colitis)
Heart Disease
(Essential hypertension, coronary artery disease, arrhythmias)
Immune Disorders
(Rheumatoid arthritis, multiple sclerosis)
Sexual and Reproductive Dysfunction
(Sexual Dysfunction ,Premenstrual Syndrome Fertility, miscarriage, etc.)
Principles of Stress treatment1, remove or diminish the stressor
2, replenish nutrients
3, non-pharmacologic methods:
acupuncture,music etc
4, teaches coping techniques
"Fight for your highest attainable aim; but never put up resistance in vain."
Some useful techniques
1.Reduce harmful environmental conditions
2.Teaches techniques by which person can develop stress tolerance.
3.Helps client maintain a positive self-image.
4.Help maintain emotional equilibrium.
5.Help client maintain or develop satisfying relations with others.
General Guidelines
- Rule One - Find your own purpose in life, that fits your own personal stress level.
- Rule Two - Control your emotional level by recognizing situations as being either life-threatening or non-life-threatening.
- Rule Three - Collect the good will and appreciation of others.
This is a general process of oxygen entering into tissue ,and cells.
This process is complex ,troubles in any part will affect the oxygen supply to cell, and lead to hypoxia
Ventilation Transfer
O2 ——>HbO2 ——> Tissue utilization
diffusion Circulatory system
Hypoxia is an extremely important and common cause of cell injury and death.
Definition
Hypoxia is a pathological process, in which O2 supply to tissues or organs is inadequate to meet the demand of cells; or the tissue cells can not make use of O2, leading to changes in functions, metabolisms and structures of cells and tissues of the body.
Anoxia:
The absence of O2 in the tissues
Hypoxemia:
A deficiency of O2 in blood
Three key points of Concept :
1. Pathological process
2. Causes
I)Can’t obtain enough oxygen
II)Can’t fully utilize oxygen
3. Changes
Metabolism
Function
Structure
Oxgen supply = CaO2× Q
Oxygen consumption =(CaO2-CvO2)× Q
Parameters of blood O2
1. Partial pressure of O2 (PO2)
PO2 is the tension caused by O2 physically dissolved in the blood.
The normal value :
PaO2 : 100mmHg (13.3kPa )
PvO2 : 40mmHg (5.33kPa )
PO2(in the air) :159mmHg
PO2(in alveolar air):104mmHg
Determinants of PO2 :
O2 pressure in the inhaled air
respiratory function
abnormal right-to-left shunt in pathological conditions(e.g. ventricular septal defect)
Ventricular septal defect a common congenital heart defect; an abnormal opening in the septum dividing the ventricles allows blood to pass directly from the left to the right ventricle; large openings may cause congestive heart failure .
2. Oxygen capacity (CO2max)
The maximal amount of O2 combined by hemoglobin (Hb) in 100ml blood.
 Fully saturated condition:
PO2:150mmHg
PCO2:40mmHg
T:38℃
Fully saturated condition:
PO2:150mmHg
PCO2:40mmHg
T:38℃
The level of Cp-O2max only depends on Hb :
① quantity of HB
② quality of HB
The normal value :
Cp-O2max = 1.34 ml/g × 15 g/dl = 20 ml/dl
3. Oxygen content (C-O2)
The actual amount of O2 in blood.
>combined with Hb : 98.5%
>physically dissolved:1.5%(can be omitted)
The level of C-O2 depends on:
①PO2
②The level of Hb (quality and quantity)
The normal value of C-O2 :
CaO2 ——19ml/dl
CvO2 ——14ml/dl
CaO2 - CvO2
(Arteriovenous Oxygen content difference)
normal value:
19ml/dl -14ml/dl = 5ml/dl
4. Oxygen saturation(SO2)
The percentage of hemoglobin present as oxyhemoglobin .
O2 content
SO2 can be calculated by : —–—–—–—–
O2 capacity
If 100ml blood contains 20ml O2 , the SO2 is 100%
when it contains 15ml O2 , how much is SO2 ?
The normal value :
SaO2—95%
SvO2—75%
The level of SO2 only depends on PO2
NOTE: When O2 content in arterial blood is 19ml/100ml, the O2 saturation is 95%, When O2 content in venous blood is 14ml/100ml, the O2 saturation is 70%.
Four parameters
1. Partial pressure of O2(PO2)
PaO2 : 100mmHg , PvO2: 40 mmHg
2. O2 content(C-O2)
CaO2 : 19ml/dl , CvO2: 14ml/dl
3. O2 capacity(Cp-O2max)= 1.34 ml/g × 15 g/dl
C-O2max : 20ml/dl
4. O2 saturation(SO2)
SaO2 : 95%, SvO2: 70%
Classification and pathogenesis
1. Hypotonic hypoxia
◆ Causes
(1) Decreased O2 pressure in the inspired air.
--- atmospheric hypoxia
①In enclosed room
② 3000 meters above sea level
(2) External respiratory dysfunctions

Peanuts, jelly or any other soft ,sweet food made from fruit juice and sugar boiled together ,used as a topping.
can cause
Paralysis of respiratory muscles, airway obstruction, asthma, emphysema, tuberculosis, pulmonary cancer, inflammation, and edema.
(3) Right-to-left shunt—Venous admixture
Some congenital heart diseases, such as ventricular septal defect, or if the foramen oval fails to close after birth.
◆ Characteristics of blood O2
PO2:↓
-O2 content :↓
-O2 capacity:
acute cases:N
chronic cases:↑
-O2 saturation:↓
NOTE: O2 content ↓(both in arterial and venous blood).
Oxygen capacity is normal in acute cases and is increased in chronic cases.
◆ Cyanosis
Cyanosis refers to a bluish color of the skin, nail beds and mucous membranes when deoxyhemoglobin concentration of blood in capillary is more than 5g per 100ml blood.
NOTE: Cyanosis is the most important clinical sign of hypotonic hypoxia.
The discolor of the skin, nail beds and mucous membrane.
Mechanism of Cyanosis
HbO2 (oxygenated Hb) ─bright red
Hb (unoxygenated Hb) ─bluish
CAUTION:
Not all the cyanosis means hypoxia
2. Hemic hypoxia (Isotonic hypoxia)
◆ Causes
(1) Anemia
The concentration of Hb is less than 9g/100ml。
Patients with severe anemia will have no cyanosis, since their unoxygenated Hb can not reach 5g/100ml
(2) Carbon monoxide (CO) poisoning
Mechanism of CO poisoning
① Hb combine with CO instead of O2 & produce carboxy-hemoglobin (CO-Hb),the CO-Hb can’t carry O2 any more.
② Hb may combine with both CO and O2 more tightly,so Hb can’t release O2 to tissues.
CO combines with Hb form carboxyhemoglobin (COHb), the color is cherry-red. The cherry-red/pink color will be visible in the skin, nail beds and mucous membrane during CO poisoning. It will have no cyanosis.
(3) Methemoglobinemia
Normal: ferrous state (Fe2+)
oxidized :ferric state (Fe3+)
Hb containing Fe3+ : methemoglobin
Appearance: Methemoglobin is brown, the patients will appear brown color.
NOTE: Many chemicals and drugs can oxidize the iron in Hb.(such as: amyl nitrite, aniline, nitrobenzene, acetanilid, phenacetin, and salicylates)
Enterogenous cyanosis
◆ Characteristics of blood O2
PO2 :N (isotonic hypoxia)
O2 content : N or ↓
O2 capacity : N or ↓
O2 saturation: N
3. Circulatory hypoxia
◆ Causes
circulatory deficiency
e.g;
embolism
shock, heart failure embolism.
atherosclerosis
thrombosis
tourniquet
Ischemic hypoxia
Stagnant hypoxia
◆ Characteristics of blood O2
PaO2 :N
C-O2 :N
Cp-O2max :N
SO2 : N
Note: Oxygen supplied for cell in unit time is inadequate.
PO2 in A and O2 content in A are normal; because when blood flow passes through tissues slowly, the PO2 and O2 content in venous blood are decreased. C(a-v) is increased.
C(a-v): ↑ blood flow passes through tissues slowly, the PO2 and O2 content in venous blood are decreased. C(a-v) is increased.
4. Histogenous hypoxia
Histotoxic hypoxia
◆ Causes
(1) Tissue poisoning
(2) cell injured by biological or physical factor
(3) vitamin deficiency ---vit B1
NOTE:The toxic agent substances include cyanide, arsenic, barbiturates.
◆ Characteristics of blood O2
PaO2 :N
CO2 :N
CO2max :N
SO2 : N
Note: In Histogenous hypoxia;
Cell can’t fully utilize oxygen
The color of skin in hypoxia
1.Anemia —————— pale
2.CO poisoning ———— cherry red
3.Methemoglobinemia—— brown
4.Histotoxic hypoxia—— rose red
Effects on body
Take “Hypotonic hypoxia” for an example
> Functional
> Metabolic
mild or chronic hypoxia: compensatory response
severe or acute hypoxia: organic dysfunction
1. Respiratory system
PaO2 > 60mmHg:no obvious changes
PaO2 < 60mmHg:compensation
decompensation
lower segment, Middle, upper segment
remain at a high level
With the changes in the horizontal axis, vertical axis did not change significantly
The slope is very steep.
2. Circulatory system
(1) In response to hypoxia
I) The heart rate increases (tachycardia),cardiac output increases,due to:
1. Myocardial contractility↑
2. heart rate↑
3. venous return↑
II) Peripheral vasodilation occurs.
(2) Pulmonary vasoconstriction
Due to: Sympathetic nerve(+)
Humoral factors :
Vasoconstrictive substance ↑↑
Vasodilative substance↑
significance? --- to maintain the VA/Q
(3) Redistribution of blood flow
sympathetic nerve(+)---- vasoconstriction
Local metabolites ----- vasodilation
(4) Capillary proliferation
hypoxia
|
VEGF ↑
|
Capillary hyperplasia
Severe hypoxia ---- decompensation
• Myocardiac systolic and diastolic dysfunction
• Pulmonary hypertension
• Cardiac arrhythmia:
• Venous return↓
Hypoxia acidosis hyperkalemia Arrhythmia
3. Hemic system
Hypoxia can stimulate the function of red bone marrow to produce more red blood cells.
4.Central nervous system
• Acute hypoxia : headache、impaired attention
• Chronic hypoxia : sleepiness, depression
• Severe hypoxia : confusion, coma, convulsion
Mechanism:
1. energy deficiency
2. acidosis
5. Cellular alterations
Adaptation
• Ability to use O2↑:
number of mitochondia increase
• Anaerobic glycolysis↑:
phosphofructokinase activity increase
• Low metabolic state:
caused by acidosis
• Myoglobin↑
Cellular damage (seen in severe hypoxia)
(1)Cell membrane
(2)Mitochondria
(3) Lysosome
Consequences at the cellular level
Lack of ATP may let the sodium pump have no activity, the result is cellular swelling. Hypoxia can increase the cell-membrane permeability, intracellular enzymes enter the ECF.
Myocardial cells contain the enzymes GOT (glutamic-oxaloacetic transaminase), LDH (lactic dehydrogenase), and CPK (creatine phosphokinase), following myocardial infarction the serum levels of these enzymes rise.
GOT and LDH are also abundant in the lungs, liver, pancreas, and kidneys.
Only the heart, brain, and skeletal muscles contain CPK.
Shock
Research history of the shock:
Some common signs:
Paleness or cyanosis
Hypotension
Cold and clammy skin
Oliguria
Dulled sensorium
Traditional view : Hypotension
Traditional treatment principle: Raise BP
Today's point of view:
modern view : low perfusion

modern treatment principle :Improve perfusion
blood pressure ×
blood flow √
Content you should know:
I.Concept
II.Classification
III.Stages and their pathological changes and mechanisms
IV.Organ dysfunction
V.Treatment principles
First of all the Concept of a Shock:
What actually shock is ?
Shock is a dangerous clinical pathological process characterized by an acute circulatory failure, inadequate blood flow and oxygen delivery to the tissue of the body.
II. Classifications of shock:
According to:
Cause
Perfusion factors
Cardiac output
Causes:
Common character :Sharp drop of the ECBV
According to the causes:
1-Hypovolemic shock
2-Burn shock
3-Traumatic shock
4-Infectious shock
5-Cardiogenic shock
6-Neurogenic shock
7-Anaphylactic shock
Perfusion Factors
Three determinants of effective perfusion

Sufficient blood volume
Normal function of heart pump
Normal vasomoter function
three types :
Hypovolemic shock
Cardiogenic shock
Vasogenic shock
Cardiac output:
◆ Hypodynamic shock (Cold Shock): inadequate or falling cardiac output
Vasoconstriction
seen in most of the shock
◆ Hyperdynamic shock (Warm shock): normal or high cardiac output
Vasodilation
seen in anaphylactic shock , neurogenic shock and part of infectious shock
III. Stages and their pathological
changes and mechanisms :
Phased basis:
The changes of microcirculation
The normal structure of microcirculation
Perfuse: Arteriole, Precapillary sphincter
Outflow: Venule
Take Hypovolemic shock as an example:
Stages:
Ischemic hypoxia Stage
↓
Stagnant hypoxia Stage
↓
Organic failure Stage
1. Ischemic hypoxia Stage:
(1) Changes of microcirculation
Decreased blood volume
↓
Sympathetic-adrenal system activation
↓ ↓
Capillary constriction Arteriovenous shunt open
↓ ↓
Tissue hypoxia
(2) Significance of compensation
1- Auto blood transfusion
Auto blood transfusion
Sympathetic-adrenal system activation
↓
constriction of the capacitance vessel
↓
Disgorging stored blood
↓
“The first-line defensive response”
2- Auto fluid transfusion
Mechanism of auto fluid transfusion
Sympathetic-adrenal system activation
↓
precapillary resistance > postcapillary resistance
 ↓
Hydrostatic pressure↓
↓
promoting tissue fluid reflow to blood
↓
Hydrostatic pressure↓
↓
promoting tissue fluid reflow to blood
“The second-line defensive response”
3- Redistribution of blood volume

Redistribution of blood volume
obvious constriction in Some organs’ vessel ,others are not
↓
ensure adequate blood flow through the brain and heart
“The third-line defensive response”
(3) Clinical Manifestation
Bp?
What are the determinants of Bp?
-Blood volume
-Heart pump
-Peripheral resistance
Mechanism of blood pressure does not drop:
Auto-transfusion
Auto-perfusion
RAAS
ADH
During the early stage of hypovolemic shock,
the patient can maintain the normal BP.
Acute or Severe blood loss and fluid loss Should be excepted
Question :
Is Bp the most important index in diagnosis and management of shock?
NO!
Other Manifestations :
Sympathetic - adrenal system activation
↓ ↓ ↓
↓ small blood vessel constriction Activation of the sweat glands
↓ redistribution of blood
↓ ↓ ↓ ↓
↓ GFR↓ ↓ ↓
↓ ↓
HR↑ Urine output ↓ cool and moist skin
How about the consciousness of patient?
clear consciousness
agitate, restless
2. Stagnant hypoxia Stage
Prolonged excitation of Sympathetic adrenal system
↓ ↓
Widespread tissue hypoxia ↓
↓
Acid metabolites produced: Endothelial cell injury
Lactic acid,Histamine,Adenosine ,NO,etc
↓ ↓ ↓ ↓
precapillary postcapillary resistance is still high permeability↑ ↓
resistance↓
↓ ↓
blood fluid slowly,Congestion < ::::::: RBC aggregation WBC rolling and block
↓ platelet aggregation and adhension
Venous return↓↓ :::: > Bp↓↓
Tissue hypoxia
↓
Acidosis and some cytokines
↓
precapillary resistance < postcapillary resistance
↓
Slow blood flow
↓
Stagnant hypoxia :::::: > vicious circle
Clinical Manifestation
Stasis in microcirculation
↓
Returned blood volume↓ Congestion
↓ ↓
CO ↓ Cyanosis
↓ ↓ ↓
Renal blood flow ↓ Cerebral ischemia
↓ ↓ ↓
Oliguria Bp ↓ coma
3. Organ Dysfunction Stage
severe hypoxia in tissue level
↓
Cell injury, Blood vessel injury ,Collagen exposure
Blood coagulation factors activation Acidosis
↓
DIC
(disseminated intravascular coagulation)
DIC is an acquired hemorrhagic syndrome
in which both clotting and bleeding occur
simultaneously. Widespread clotting in small
vessels leads to consumption of the clotting
factors and platelets, which in turn leads
to bleeding.
DIC <::::::::> shock
MSOF----multiple system organ failure
MODS is the progressive dysfunction of two or more organ systems resulting from an uncontrolled inflammatory response to a severe illness or injury.
Review
Ischemic hypoxia Stage
↓
Stagnant hypoxia Stage
↓
Organic failure Stage
IV. Organ dysfunction
1. Shock lung
Shock lung or the adult respiratory distress syndrome (ARDS) is a form of respiratory failure that can follow severe shock. Alveolar capillary permeability is increased and interstitial edema develops, the lung becomes engorged and gas exchange is impaired, hyaline membrane develops.
Shock lung
Rapid and labored respiration
PaO2↓
Diffusion impairment
Ventilation-perfusion imbalance
2. Acute renal failure
Renal failure
- Oliguria
- Azotemia
- Hyperkalemia
- Metabolic acidosis
Functional renal failure
Parenchymal renal failure
 3. Heart failure
3. Heart failure
Heart failure
- Acidosis
- Hyperkalemia
- Decreased PO2
- DIC
- Endotoxin
4. Gastrointestinal dysfunction
ischemic injury
redistribution of blood flow
DIC
Endotoxin
↓
Gastric mucosal damage, intestinal ischemia and stress ulcer
↓
Clinical manifestation:
Abdominal pain
Vomiting blood
Blood in stool
V. Treatment:
Shock is easier to prevent than to cure.
Don’t wait for symptoms to develop before beginning the treatment for shock.
prevention first
1. Blood and Plasma transfusion:
Lose?
The amount is based on how much patients do
Need?
2. Vasoactive Drugs:
Note: a precondition
expansion of blood volume
Vasodilator substance.
Vasoconstrictive substance.e.g;
neurogenic shock
anaphylactic shock
3-Other treatment measures:
-Oxygen therapy
-treatment on acidosis
-treatment by the head-down position
-treatment with glucocorticoids
Questions just for review!
1. What is the concept of shock?
2. What are the major causes of shock?
3. How many stages are there in hypovolemic shock? What are they?
4. What are the compensatory mechanisms and significance in first stage of hypovolemic shock?